
Is There a ‘Most Optimal’ Treatment for Frozen Shoulder?
Reference
Rangan, A., Brealey, S., Keding, A., Corbacho, B., Northgraves, M., & Kottam, L. et al. (2020). Management of adults with primary frozen shoulder in secondary care (UK FROST): a multicentre, pragmatic, three-arm, superiority randomised clinical trial. The Lancet, 396(10256), 977-989. https://doi.org/10.1016/s0140-6736(20)31965-6
Objective
Apart from conventional physiotherapy, manipulation under anaesthesia and arthroscopic capsular release are two alternative treatment methods for frozen shoulder. However, they tend to be more invasive and costly. There is also limited evidence to suggest that those two interventions are superior to regular physiotherapy with steroid injection. Hence, the purpose of this study is to directly compare and investigate which of the three interventions is more optimal in improving shoulder function and pain.
What They Did
Inclusion criteria:
- 18 years or older
- has clinical diagnosis of unilateral frozen shoulder
- characterised by the restriction of passive external rotation in the affected shoulder to less than 50% of the opposite shoulder
Exclusion criteria:
- bilateral concurrent frozen shoulder
- frozen shoulder secondary to trauma or secondary to other causes (eg, recent breast surgery)
- Diabetic patients were included, because this is significantly associated with impaired shoulder mobility in this patient population
- unfit for the interventions used for the study (e.g. anaesthesia or corticosteroid injection)
By random assignment, 189 participants received manipulation under anaesthesia*, 191 received capsular release**, and 93 received early structured physiotherapy***
Outcome measures:
Primary:
- Oxford Shoulder Score
Secondary:
- Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH)
- Numeric Rating Scale for pain;
- Perceived extent of recovery
- measured by a single visual analogue scale (VAS) ranging from 0 (no need to seek further treatment) to 100 (definite need)
- input from both patient and clinician
- Cost effectiveness
All outcome measures were collected at baseline, 3 months, 6 months, and 12 months after randomisation.
*surgeon manipulated the affected shoulder to stretch and tear the tight capsule while the participant was under general anaesthesia, supplemented by a steroid injection. Twelve sessions of conventional physiotherapy was provided afterwards.
**surgeon surgically divided the contracted anterior capsule in the rotator interval while participant was under general anaesthesia, followed by manipulation with optional steroid injection. Twelve sessions of conventional physiotherapy was provided afterwards.
***mobilisation techniques and a graduated home exercise programme supplemented by a steroid injection.
What They Found
OSS score
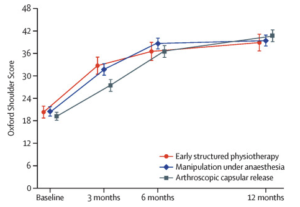
- Arthroscopic capsular release led to significantly higher OSS scores than those assigned to manipulation under anaesthesia (40·3 vs 38·3 points) or to early structured physiotherapy (40·3 vs 37·2 points).
- Manipulation under anaesthesia had higher mean OSS scores than the early structured physiotherapy group (38·3 vs 37·2 points).
- However, mean estimates were less than the MCID of 4–5 OSS points, suggesting that the differences are not clinically significant.
QuickDASH and shoulder pain
- Capsular release group has significantly poorer outcomes 3 months but better outcomes at 12 months when compared with manipulation or early physiotherapy.
Perceived extent of recovery
- No statistically significant difference found between all 3 groups.
Number of further treatment required
- Physiotherapy with anaesthesia required the most amount of further treatment (19), followed by manipulation under anaesthesia (15) and capsular release (8).
Cost effectiveness
- Manipulation was £276·51 more expensive per participant than was early structured physiotherapy.
- Capsular release was substantially more costly than physiotherapy (on average £1733·78 more per participant) and manipulation (on average £1457·26 more per participant)
- Capsular release had worse QALYs than did manipulation under anaesthesia
- Manipulation had better QALYs than did physiotherapy
- Manipulation was the intervention most likely to be cost-effective at a threshold of £20 000 per QALY
Adverse events
- ten serious adverse events were reported for nine (2%) of 503 participants
- eight (4%) of 203 in the capsular release group
- two (1%) of 201 in the manipulation group
- 33 non-serious adverse events were reported for 31 (6%) of 503 participants, with similar rates in the three groups (no evidence of statistical differences in proportion)
Conclusion
All three treatments showed substantial improvements in patient-reported shoulder pain and function. None of them were clinically superior. Arthroscopic capsular release resulted in the least number of further treatments but carried higher risks and much higher costs. The early structured physiotherapy with steroid injection had more patients who needed further treatment, making manipulation under anaesthesia the most cost-effective treatment (at a threshold of £20 000 per QALY)
Practical Takeaways
It appears that surgical procedures have similar clinical outcomes when compared to early physical therapy. For patients who wishes to shorten the number of follow-up treatment and is able to afford the higher costs, capsular release is a good option. Conversely, for patients who prefers more conservative treatment method and is comfortable with longer follow-up duration, early structured physiotherapy with steroid injection is an ideal intervention to recommend. Manipulation under anaesthesia is suitable for patients who desires the most cost-effective treatment in terms of QALYs per dollar spent.