Which Exercise Protocol is Best for Jumper’s Knee?

Reference
Lim, H., & Wong, S. (2018). Effects of isometric, eccentric, or heavy slow resistance exercises on pain and function in individuals with patellar tendinopathy: A systematic review. Physiotherapy Research International, 23(4), e1721. https://doi.org/10.1002/pri.1721
Objective
Traditionally, eccentric training has been the first-line of treatment for patellar tendinopathy. However, the protocol advises patients to use relatively heavy weights to load the tendon up to a pain level of 5/10, which may be inappropriate for in-season athletes who already doing high volumes of sport-specific training. Some studies have found that isometric exercises may be superior to eccentric training in improving pain and knee function in the short-term. Other researchers have also questioned the rationale behind isolating eccentric movements, since protocols such as Heavy-Slow Resistance (HSR) training, which includes both concentric and eccentric movement, has been shown to produce similar benefits.
Thus, this systematic review aims to assess the efficacy of eccentric, isometric and HSR training in improving pain and function for patellar tendinopathy.
What they did
The researchers included studies that used either isometric, eccentric or HSR training as treatment, and uses pain and/or knee function as the outcome measure. They excluded studies that involved invasive interventions, such as surgery and injections. Quality of studies were rated to be moderate to high. 15 studies were selected in total, 3 were on isometric training, 2 on HSR training, 10 on eccentric training. Number of participants added up to 310. 55 were in isometric training, 27 in HSR training, 228 in eccentric training.
What they found
Pain
- Isometric
- Both Isometric and isotonic training produced pain relief immediately, but only isometric training continued to produce pain relief at 45mins post-intervention. Isometric training also produced greater reduction in pain intensity compared to isotonic training. However, there is no difference in pain score in the mid to long term.
- HSR
- HSR seems to improve pain for up to 12 weeks, but this is based on within-subject differences (i.e. no statistical comparison with control group)
- Eccentric
- Based on within-subject differences, there were mixed findings in pain reduction. When eccentric training was compared to passive treatments such as manual therapy and ultrasound, all participants in the former group experienced pain reduction, but only 20% of participants in latter group experienced pain relief.
Knee Function
- isometric
- Both isometric and isotonic groups had improvements in knee function (based on VISA score)
- HSR
- HSR improves knee function up to 12 weeks post-intervention (based on VISA score). Improvement in countermovement jump height was also observed 70% of participants undergoing HSR.
- Eccentric
- There were mixed findings in terms of between-subject improvement in knee function (based on VISA score). Stretching with eccentric training seems to improve knee function compared with eccentric training alone. When compared to regular squat exercise, eccentric training led to greater number of athletes returning to sports.
Level of Recommendation
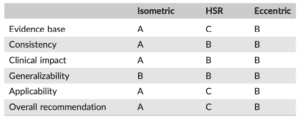
- Grade A: evidence can be trusted to guide practice
- Grade B: evidence can be trusted to guide practice in most situations
- Grade C: evidence provides some support for recommendation(s), but care should be taken in its application.
Limitations
No direct statistical comparison could be made between the different exercise protocols, due to the heterogeneity in the research design of the selected studies. Also, there were far fewer number of studies representing HSR (2) and isometric training (3) in this review, compared to eccentric training (10).
Conclusion
Isometric training is superior to HSR and eccentric training for short-term improvement in pain. However, HSR and eccentric training produces longer-lasting improvement in pain and knee function compared to isometric training.
Practical takeaways
Given that isometric training is effective in producing rapid pain relief, this makes it a suitable intervention for athletes who are in-season and have lesser downtime available. Eccentric and HSR training may be better suited for athletes in their off-season, when there is a longer buffer time to improve knee function.
Eccentric exercises might be more cumbersome to perform, given that the unaffected leg needs to assist in the concentric portion of every rep. Hence, patients with lower skill level or unaccustomed to exercising might find HSR more straightforward.
However, it is also worth noting that only 2 studies on HSR were included compared to the 10 studies on eccentric training. If HSR training did not lead to improvements, eccentric training can be considered given that it has a good track record in managing tendinopathy.